



科室医生 查看全部







科普·直播义诊专区 查看全部
- 精选 膝关节骨性关节炎阶梯化治疗的新进展(2023)
膝关节骨性关节炎阶梯化治疗的新进展(2023)骨性关节炎(osteoarthritis,OA)是一种严重影响患者生活质量的关节退行性疾病,而膝关节骨性关节炎(kneeosteoarthritis,KOA)在临床最常见,主要表现为膝关节疼痛和活动受限。膝关节骨性关节炎是发病率最高、临床最常见、病程长、阶梯性明显、对个体和社会损害最大的骨关节炎之一。由于种种原因,目前我国各地区、各级医院骨科诊疗水平发展不均衡,关节疾病的诊疗水平参差不齐,对膝关节骨性关节炎的诊疗缺乏系统性的培训、全面深入的认识,难以对膝关节骨性关节炎患者严重程度进行恰当判断,易导致不适合治疗或诊疗延误。有鉴于此,查阅国内外最新文献,聚焦对膝关节骨性关节炎阶梯化治疗:基础治疗、药物治疗、修复性治疗和重建治疗四个层次,经过充分细致、广泛深入、独立客观、科学循证的文献分析,总结形成膝关节骨性关节炎阶梯化治疗的图文并茂、容易理解掌握的新进展。以期本新进展为医务人员对膝关节骨性关节炎阶梯化的治疗工作,提供科学、规范、有效的参考。新进展的全文请见PDF文档。
 曾纪洲 主任医师 北京潞河医院 骨关节外科193人已读
曾纪洲 主任医师 北京潞河医院 骨关节外科193人已读 - 非外伤性股骨头坏死发病机制的ARCO共识(2021)
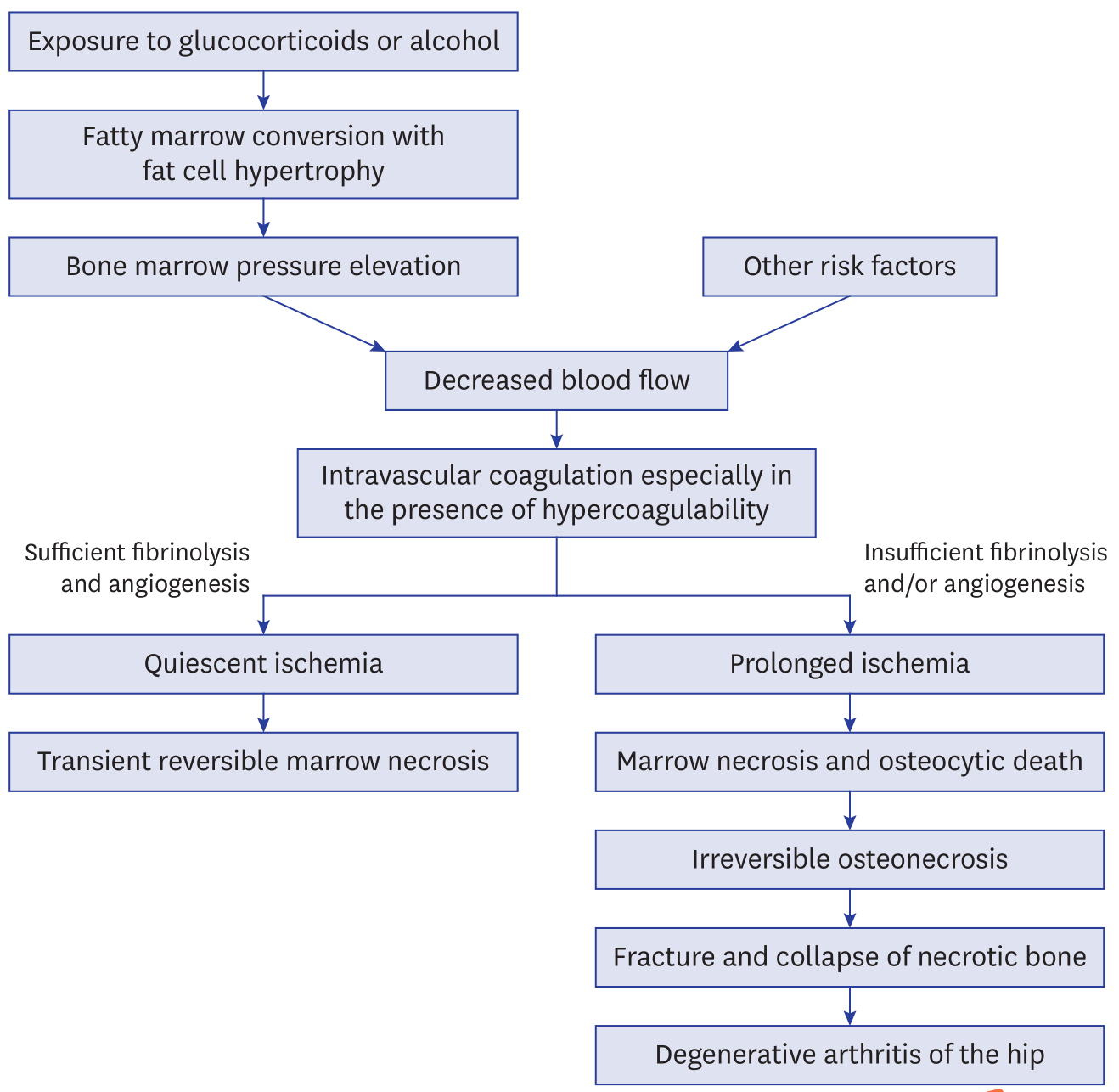
非外伤性股骨头坏死发病机制的ARCO共识(2021)ARCOConsensusonthePathogenesisofNon-traumaticOsteonecrosisoftheFemoralHead CuiQ,JoWL,KooKH,ChengEY,DrescherW,GoodmanSB,HaYC,HernigouP,JonesLC,KimSY,LeeKS,LeeMS,LeeYJ,MontMA,SuganoN,TaliaferroJ,YamamotoT,ZhaoD.ARCOConsensusonthePathogenesisofNon-traumaticOsteonecrosisoftheFemoralHead[J].JKoreanMedSci,2021,36(10):e65. 转载文章的原链接1:https://pubmed.ncbi.nlm.nih.gov/33724736/ 转载文章的原链接2:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7961868/ AbstractOsteonecrosisofthefemoralhead(ONFH)isadevastatingdiseasefrequentlyleadingtofemoralheadcollapseandhiparthritis.Specifically,non-traumaticONFHprimarilyaffectsyoungandmiddle-agedadults.Althoughcompromisedlocalcirculationofthefemoralheadseemstobepathognomonicforthedisease,thepathogenesisisperplexingandcontinuestobeanareaofscrutinyandresearch.Comprehensionofthepathogenesisisofcrucialimportancefordevelopingandguidingtreatmentsforthedisease.Therefore,weprovideanup-to-dateconsensusonthepathogenesisofnon-traumaticONFH. Keywords:Pathogenesis,Osteonecrosis,OsteonecrosisoftheFemoralHead GraphicalAbstract INTRODUCTIONOsteonecrosisofthefemoralhead(ONFH)isaconditioninwhichpartofthefemoralheadbecomesnecroticassociatedwithadisruptionofthebloodsupply.1Thenecrosisusuallyinvolvestheweight-bearingdomeofthefemoralhead.Asthediseaseprogresses,mechanicalstrengthofthenecroticboneisreduced,leadingtoeventualcollapse.Thissubsequentlyleadstosecondaryarthritisofthehip.OnecommoncauseofONFHistrauma.Adisplacedfemoralneckfractureorhipdislocationcaninjurethelocalbloodvesselsandleadtobonedeath.Non-traumaticriskfactorsforONFHincludetheuseofcorticosteroids,excessivealcoholintake,excessivetobaccouse,sicklecelldisease,systemiclupuserythematosus,organtransplantation,humanimmunodeficiencyvirusinfection,coagulopathies,anumberofgeneticfactors,Caissondisease(deep-seadivers),myeloproliferativediseases(marrowpackingdiseases),andradiationnecrosis.2,3,4 Non-traumaticONFHusuallyaffectsadultsyoungerthan50yearsandfrequentlyprogressestocollapseofthefemoralhead.IntheUnitedStates,about10,000newpatientsareestimatedtobeaffectedwiththediseaseannually.5TheannualincidencerateinJapanwas1.91/100,000andtheannualincidencewasestimatedtobemorethan2,400in2015.6InSouthKorea,theestimatedprevalenceofONFHincreasedfrom9,870in2002to18,691in2006.7Inarecentlarge-scaleepidemiologicalsurveyinChina,thecumulativenumberofpatientswithnon-traumaticONFHreached8.12millionamongtheChinesepopulation.8Therehasbeenconsiderableprogressmadeonourcomprehensionconcerningthepathogenesisofthenon-traumaticONFHduringthelast3decades.However,moststudiesreportfragmentaryknowledgeandanintegratedexplanationofthepathogenesishasnotbeenestablished.9Thus,theAssociationResearchCirculationOsseous(ARCO)taskforcemembershavesystematicallyreviewedtheup-to-dateknowledgewiththisreportrepresentingaconsensusonthepathogenesisofONFH. ARCOTASKFORCEANDPREPARATIONOFTHEMANUSCRIPTInApril2020,theARCOtaskforcewasestablishedincluding4members:3orthopedicsurgeonsand1rheumatologist.TheythoroughlysearchedPubMedandreviewedofrelevantarticlesaboutthepathogenesisofnon-traumaticosteonecrosisofthefemoralhead.Thesearchwasdoneusingthekeysearchterms“osteonecrosis,”“avascularnecrosis,”“asepticnecrosis,”“pathology,”and“pathogenesis”forentriesfromJanuary1,1970toMarch31,2020.Afterthen,thetaskforcepreparedthefirstdraftandcirculateditto14ARCOmembers.ThemanuscriptwasrepeatedlyreviseduntilallparticipantsagreedanditwasfinalizedinSeptember2020. HISTOLOGICCRITERIAOFONFHArletandDurrouxdescribedONFHasaprogressivediseaseinvolvingthemarrowspacefirst,followedbythetrabecularbonelater.Theyclassifiednecroticlesionsinto4types10:Type1lesionsshowlossofhematopoieticcellsinthemarrowandfattymarrowconversion;Type2lesionsdemonstratenecrosisofthemarrow;Type3lesionsexhibitnecrosisofthemarrowandbone(deathofosteocytes>50%);andType4lesionsdemonstratenecrosisofthemarrowandbonewithencapsulatingfibrovasculartissue,whichchangestoscleroticbonelaterbyappositionofnewbone.Type2lesionsarenon-specificforONFHastheyareseeninotherpathologiesincludingtransientbonemarrowedemasyndrome(BMES),11,12theuninvolvedfemoralheadsofpatientswhohaveunilateralONFH,13andthefemoralheadsofpatientswhoaretreatedwithcorticosteroids.14,15,16,17Thepresenceoftype4lesionisgenerallyacceptedasahistologiccriteriontomakeadiagnosisofONFH.16,18,19 CURRENTCONCEPTSCONCERNINGTHEPATHOGENESISOFONFHCurrently,threetheoriesaregenerallyacceptedintermsofthepathogenesisofONFH.Thefirsttheoryconsidersboththeboneandintravascularmechanismsasthecause.2,16,20,21Thesecondtheoryconsidersonlyintravascularcoagulationasthepathwaytoischemia.2,16,20,21ThethirdtheorypromotesONFHashavingamultifactorialetiology.1,2,3,4,5Inmostcases,ONFHisassociatedwithmultiplefactorsincludinggeneticpredispositionsaswellastheexposuretoriskfactors.AnyoftheriskfactorscanplayaroleinthedevelopmentofONFHandcontributetoitspathogenesisinmostcases.22,23,24,25,26,27,28,29Thehereditarypredispositionexplainwhyonlysomeofthehigh-dosecorticosteroidsusersandalcoholabusersacquirethedisease,whileothersdonot.Indeed,anischemiceventdoesnotalwaysleadtoONFH.Theprogressionisgenerallydependentontherestorationofvascularperfusionandthecreepingsubstitutionofdeadbonebynewbone.2,16,20,21 In1949,ChandlertermedONFH(thencalledavascularnecrosis)as“coronarydiseaseofthehip”becausehethoughtthatthecausewasanabruptvascularobstructionbythrombosisorembolism.30However,unlikethecoronaryartery,thelateralepiphysealvesselsarehousedwithintheclosedchamberofthefemoralhead,whichisfilledwithmarrowcells.Therefore,femoralheadosteonecrosisshouldbeconsideredasacompartmentsyndromeofthefemoralheadduetointra-osseoushypertensionratherthanasavascularobstructivedisease,althoughthisisdebatable.10 Therearesufficientdatatosupportsuchapathophysiologiccascade:fatcellhyperplasia;intra-osseoushypertension;vascularcompressionandthrombosis;ischemia;marrowandbonenecrosis;subchondralfracture;andcollapseofthefemoralhead,particularlyincorticosteroid-andalcohol-associatedONFH,whileotherriskfactorsmayworkthroughdifferentmechanisms.Thisleadstosubsequentsecondaryarthritisofthehip;theend-stageofONFH(Fig.1).16,19 Fig.1Pathogenesisofnon-traumaticosteonecrosisandtransientmarrownecrosis. Fatcellhypertrophyinthemarrowspaceandintra-osseoushypertensionCorticosteroidspromotedifferentiationofpre-adipocytesandmesenchymalstemcellstomatureadipocytesbystimulatingtheperoxisomeproliferator-activatedreceptor-gamma(PPAR-γ)andsuppressingrun-relatedtranscriptionfactor2(RUNX2).31,32,33,34,35,36Inaddition,corticosteroidsandalcoholinduceadipocytehypertrophythroughincreasinglipidsynthesisofthemarrowfatcell.31,32,33,34,35,36Severalpolymorphismsingenesinvolvedincorticosteroidmetabolism(adenosinetriphosphatebindingcassetteB1,ABCB1)orinlipidmetabolism(apolipoproteinB,ApoB)areassociatedwithONFH.37,38Hematopoieticcellsaredepletedandthemarrowspaceisfilledwithlarge(>10µm)roundtoovoidfatcells(ArletandDurrouxType1lesion)(Fig.2).33,34,35 Fig.2Themarrowspaceisfilledwithhypertrophiedfatcells.However,osteocytesareseeninlacunae(ArletandDurrouxType1lesion)(hematoxylinandeosinstain,originalmagnification×200). Duetothefattymarrowconversion,theproximalfemoralmetaphysisshowsahighsignalintensityonT1-weightedmagneticresonanceimages(MRIs).39Theincrementofmarrowfatcellvolumeand/oranincreaseinthenumberoffatcellsinduceintra-osseoushypertensionintheproximalfemur.Theintra-osseoushypertensioncompressesvenoussinusoids,leadstointravenousmicrovascularcoagulationandsubsequentimpairmentofbloodflowtothefemoralhead.39,40,41,42 MarrownecrosisIntravascularcoagulationleadstoacuteischemiainthemarrowofthefemoralhead.Normalmarrowcavitiesarepredominantlyfilledwithtwotypesofcells;bonemarrowfatcellsandhematopoieticcells.Themarrowfatcellaccountsforapproximately70%oftheadultbonemarrowvolume.Thenumberofhematopoieticcellsgraduallydecreaseswithage.Eachmarrowcellhasdifferenttolerabilityforischemia.43,44,45,46Thehematopoieticcellsaresensitivetotheischemiaandmostofthemwilldiewithin12hoursaftertheischemicevent.46Themarrowfatcellssubsequentlydieandtheirnucleidisappearwithin48hoursofacompleteischemia.Thus,theinitialmicroscopicsignsofboneischemiaappearinthemarrowspace.Thehematopoieticcellsdisappearandthenthefatcellsbecomenecrotic(ArletandDurrouxType2lesion)(Fig.3). Fig.3Nucleioffatcellsarenotseenandthemarrowspaceisnecrotic.However,morethan50%ofthelacunaearefilledwithosteocytes(ArletandDurrouxType2lesion)(hematoxylinandeosinstain,originalmagnification×200). Thrombophilia/hypofibrinolysisandimpairedangiogenesisIntravascularcoagulationthatoccurswithinthefemoralheadtriggersfibrinolysis.Thefibrinolyticsystemisbuiltuponactiveenzymes,proplasmin,andaserineproteasethatdegradesfibrinclots.Variousgeneticandhereditaryconditions,whichcauseincreasedthrombosisand/ordecreasedfibrinolysis,accentuateand/orprolongtheintravascularcoagulation.Severalcoagulopathieshavebeenimplicatedincausingthisintravascularcoagulation.ProteinChasananticoagulantcapacitybycorruptingprocoagulantfactorsVaandVIIIa.ProteinSservesascofactorfortriggeredproteinC.41ProteinsCandSdeficiencies,47,48,49,50,51aswellasmutationsinthefactorVLeidenortheprothrombin20210Agene,51increasethrombosis.Polymorphismsoftheplasminogenactivatorinhibitor-1gene(PAI-1)areassociatedwithahypercoagulablestate.49,52,53Antiphospholipidantibodies,54,55inflammatoryboweldisease,56,57andsicklecelldisease58,59alsoincreasetheriskofmicrovascularthrombi.Moreover,arecentgenome-wideassociationstudyfromJapanidentifiedlongintergenicnon-proteincodingRNA1370(LINC01370)asacandidateriskgeneinJapanesepatientswhohaveidiopathicONFH,andstratifiedtheiranalysisbyriskfactorssuggestedthatthe12q24locuswasassociatedwiththediseasethroughdrinkingcapacity.60Thisintravascularcoagulationleadstolocalhypoxia,nutrientdeficiency,andmarrownecrosis,whichultimatelyactivatesangiogenesis.CompromisedangiogenesishasbeenconsideredasacontributingfactorforthedevelopmentofONFH.Nitricoxide,aknownvasodilator,advancesangiogenesisandboneformation.Polymorphismintheendothelialnitricoxidesynthase(eNOS)genehasbeenrelatedtoONFHinpatientswhohavenoacquiredriskfactors.24,29Vascularendothelialgrowthfactor(VEGF),whichispromptedbyhypoxia,isaknownangiogenicproteinthatalsopromotescartilageandboneregeneration.GeneticpolymorphismsofVEGFarerelatedtotheprogressionofcorticosteroid-associatedONFH.26,28CorticosteroidsalsoinhibitangiogenesisbysuppressingtheproductionofVEGF.61Ifcompletefibrinolysisandadequateangiogenesisoccurwithinthecriticalischemicperiod,thedurationofischemiacanbebriskandthebloodperfusioncanberestored.Althoughthemarrowspaceremainsfatty,thelesionisreversibleanddoesnotprogresstodefiniteosteonecrosis.16Mostosteocytes(>50%)remainviable(ArletandDurrouxtype2or3lesion).Theischemiadoesnotproduceasequestrumandthereisnofibrovascularreparativezonearoundthenecroticmarrow.Thereactiveband,whichistheearliestdiagnosticmagneticresonance(MR)findingforONFH,62isnotseen.TheonlynonspecificMRfindingisanincreaseinsignalintensityoftheproximalfemoralmetaphysisonT1-weightedimages,whichindicatesanincreaseoffatsubstanceinthemarrowspace. OsteocyticdeathandformationofasequestrumInthepresenceofthrombophilia/hypofibrinolysisand/orimpairedangiogenesis,prolongeddamageduetoischemiaoccursanddefiniteONFHdevelops.Aftercompleteischemia,osteocytesstarttodisappearwithin24to72hoursandafocalsequestrumisformed(ArletandDurrouxType3lesion)(Fig.4).46,63,64,65Onceasequestrumisformed,thecourseofthediseaseisirreversible. Fig.4Marrowisnecroticandmostlacunaeareempty(ArletandDurrouxType3lesion)(hematoxylinandeosinstain,originalmagnification×200). ReparativeprocessatthemarginofthesequestrumNecroticbone,whenrecognizedasaforeignbodybythehost'simmunesystem,inducesanimmunereaction.Thehistocompatibilityantigensofdeadbonearetheglycoproteinsoncellsurfaces.Thesematrixproteinsmayormaynotelicitaforeignbodyreaction.Thehostresponsetodeadbonedependsontheconcentrationandtotaldoseoftheantigenofthedeadbone.26Necroticboneisacompositematerial,whichhasmanyantigensofglycoproteinsandpotentiallycouldelicitvaryingimmuneresponses.Hydroxyapatiteinthetrabeculaeelicitsaminimalimmuneresponse.ExtracellularcompositessuchastypeIcollagenandnon-collagenousmatrixproteins(i.e.,proteoglycans,osteocalcin),induceamildimmunereaction.However,byproductsfromdeadbonemarrowcellscanelicitamoremarkedimmuneresponse.61Thenecroticboneisencapsulatedbyafibrousmembrane,definedhistologicallyasareactivezone.OnMRIs,thisappearsasabandoflow-signalintensity.AdefinitediagnosisofONFHismadeatthisstage,whichischaracterizedbytheformationofafocalsequestrumsurroundedbyafibrousmembrane.13,19Marrowedemacanbeassociatedwiththeviableportionaroundthesequestrum.Theedemaincreasesthebonemarrowpressure,whichmayleadtosymptomaticpaininthepatient'ship.66Capillariesinfiltrateintothefibroticcapsule.However,thisangiogenesisisstoppedatthemarginofthesequestrum.Thereparativefibrovasculartissuecannotpenetrateintothedeadmarrowspaceofthesequestrumandlittletonobiologicalrepairoccursinthenecroticportionofthefemoralhead.67Thefibroticcapsuleisprogressivelyossifiedandappearsasascleroticrimonradiographs.Boneturnoverinthisstepisalsoaffectedbysomegeneticpredispositionsuchasmatrixmetalloproteinases,osteoprotegerin(OPG),andreceptoractivatorofNF-κBligand(RANKL).68,69,70 SaponificationofnecroticboneandsubsequentfractureThereisnobiologicalreactioninthenecroticportionduetotheabsenceofbloodsupply.However,deadmarrowundergoesachemicalchange,initiatedbydeadadipocytesreleasingfattyacids.71Thesefattyacidssaponifywithextracellularcalciumtoforminsolublesoaps.72,73SaponifiedmarrowshowsupasaMitchellclassDlesionwithadarksignalonMRIs.74Thedeadtrabeculaeandsaponifiedmarrowdonotachievethesamemechanicalstrengthandstructuralintegrityofpreviouslyhealthybone.Fatiguefracturesoccuratthesubchondralportionofthejointduetothislossofstructuralintegrity.Thesefracturesappearonradiographsasthe“crescent”sign.Fracturesalsoformatthenecroticmargininsidetheossifiedreactiveregion.Thesubchondralfractureleadstocollapseofthefemoralheadandsubsequentarthritisofthehip(Fig.5). Fig.5Fibrousencapsulation(arrows)isseenattheperipheralportionofthesequestrum(ArletandDurrouxType4lesion).Subchondralfracture(arrow-heads),whichappearsasthe“crescent”signonradiograph,isseen(hematoxylinandeosinstain). TRANSIENTBMESTransientBMESisanuncommondiseaseofthehip,whichcommonlyrecoversspontaneouslywithinseveralmonths.12,75,76,77,78,79,80Itsetiologyandpathogenesisremainunknown.However,ischemiahasbeensuggestedasacauseofthediseaseasthehistologicfindingsofBMESaresimilartothoseseeninthemarrowoftheearlystagesofONFH,12,76,77andthereforeitisbrieflydiscussedheretogetherwithONFH.SomepregnantwomendevelopBMESintheirthirdtrimester75,78andanassociationwithhypofibrinolysiswasreportedinfamilialBMES.79,80However,mostBMESpatientsdonothaveriskfactorsforONFH.12,66,67,72,73,74,75,76,77Intravascularcoagulationandmarrownecrosismayoccurintheabsenceorpaucityofriskfactors.InBMES,thefateofthefemoralheadaftertheischemiceventisquitedifferentfromONFH.Completefibrinolysisandreactivevasodilatationoccur.81Thereisonlyashortperiodofsubthresholdischemichypoxia,whichisnotsevereenoughtoinducecompletebonedeath.Themarrownecrosisinducesreactivehyperemiaandincreasedvascularpermeabilityleadingtointerstitialedemainthemarrowspace.Althoughthemarrowspaceisnecrotic,mostosteocytesremainviableandmostlacunaearefilledwithosteocytes.Thereisnosequestrumformationandnoreactivezonearoundthenecroticlesion.12,77Themarrowspaceisfilledwithliquid.BytheArletandDurrouxclassification,theselesionsaretype2ortype3lesions(Fig.6).Duringtheedemaperiod,bonemarrowpressureisraised.Mostpatientssufferseverehippainandtheyarediagnosedatthisstage.Thebonemarrowedemaappearsasalow-signalonT1weightedMRIsandahigh-signalonT2weightedimages.82 Fig.6Bonetrabeculaearethinandlinedbyosteoblasts.Focalboneresorptionisseenatsomeareas(arrows).However,activeosteoclastsarenotseenandthereisnocreepingbonesubstitution.Marrowspaceisfilledwithserosanguinousmaterials,chronicinflammatorycells,vascularchannels,andfibrosis(hematoxylinandeosin,×100). Angiographyindicatesarterialdilatationandbonescansshowincreaseduptakeintheproximalfemur.Theincreasedperfusioninducestransientdemineralizationofthetrabeculaeandcorticalboneoftheproximalfemur.Whenthedemineralizationismarked,theradiodensityoftheproximalfemurisdiminished;thishasbeenreferredtoas“transientosteoporosisofthehip”.12However,thevolumeofbonemassismaintainedandonlythemineralcontentintheboneisdecreased.Thus,theterm“osteoporosis”isamisnomer.Wilsonetal.82proposedtousetheterm“transientBMES”insteadof“transientosteoporosis.”Thenecroticmarrowtriggerscreepingsubstitution;bloodvesselsbegintopenetratethenecroticmarrow.Immaturewovenboneisdepositedonthesurfaceoftrabecularbone.Astheintraosseousvascularityandperfusionreturntonormal,themarrowedemaresolvesandtheosteoidismineralized.Therefore,transientBMES,unlikeONFH,isaself-limitingdiseaseanddoesnotprogresstoONFH(Fig.1).83 DISCUSSIONOurunderstandingofONFHandtheeffectsoftrauma,medications,aswellasgeneticandpatientfactorshavechangedoverthepast3decades.Recentstudieshavedemonstratedthatcorticosteroidsandalcoholpromoteadipogenesis脂肪生成inthemarrowspace,butinhibitosteogenesis骨生成andangiogenesis血管生成.35,36,84Geneticfactorsincludingthrombophilia血栓形成倾向,hypofibrinolysis低纤溶,andimpairedangiogenesis受损的血管生成alsoplaycriticalrolesinthepathogenesisofONFH.29However,thepathophysiologyofONFHismultifactorialandpoorlyunderstood.Themultisystemiceffectsofhereditaryandacquiredriskfactorsandtheirinteractionsmakethepathologicalmechanismsmorecomplicated.Auniformconceptofthepathophysiologyofosteonecrosisisvascularocclusionandischemiaofboneleadingtobonedeath.Themechanicalinterruptionofcirculationtothefemoralheadafterhipdislocationsorfemoralneckfracturesisthemostobviouspatho-mechanism.CellularorgasembolizationinthesinusoidsprobablyplaysthecentralroleofbloodsupplyocclusioninGaucher'sdisease,hemoglobinopathies,anddysbaricdisorders.However,thepathogenesisofalcohol-orcorticosteroid-associatedosteonecrosisislessclear.Marrowfatcellhypertrophywassuggestedtocontributetothepathogenesisbycompressionofthesinusoidalvascularbed,whichcausesvenousstasisandelevatedintraosseousmarrowpressure.34Sincethemarrowcavityisacompartmentencasedbyanon-expandableshellofbone,attentionhasbeenfocusedonelevatedintraosseouspressure(IOP)asapathogenicmechanism.AnelevatedIOPwithintheosteonecroticfemoralheadanddecreasedvenousdrainageandstasishavebeenshown.40OtherobservershavenotfoundIOPmeasurementstobereproducible,specific,orsensitiveforthediagnosisofosteonecrosis.14,85,86,87ElevatedIOPisobservednotonlyinosteonecrosis,butalsoinosteoarthritisandcanalsoberelatedtoelevationsinintra-articularpressureandcompressiveloads.88,89Thus,elevatedIOPdoesnotseemtobecausallyrelatedtothepathogenesisofosteonecrosisandisanonspecificandsecondary,butpotentiallycontributory,factorinthepathogenesisofosteonecrosis.Furtherstudiesarenecessaryinordertoidentifynotonlytheprecisemechanismsofthedisease,butalsopatientsatriskfordevelopingONFH,leadingtoearlypreventionandtreatment.SubchondralfractureseemstobethepointofnoreturninthediseaseprogressionofONFH,19butneedstobedifferentiatedfrominsufficiencyfractureandtransientbonemarrowedemasyndrome.MRIisusefultoruleouttheseconditions.Variouspharmacologicaltreatments;enoxaparin,statins,bisphosphonates,iloprost,andacetylsalicylicacidhavebeengiventopreventONFHinpatientsatriskortoretardthediseaseprogressioninearly-stagediseasewithoutsubchondralfractureorcollapseofthefemoralhead.However,theireffectivenessremainscontroversialandnoneofthemwereproventobeeffectivebyhigh-levelstudies.Atthismoment,nopharmacologicalpreventionortreatmentofONFHisrecommended目前,尚无针对ONFH的药物预防或治疗的推荐。.90CoredecompressionhasbeenperformedtotreatONFHundertheassumptionthatitreducesintraosseouspressure,allowsrestorationofbloodflow,regeneratesnecroticbone,andthuscancontrolorreversethediseaseprocess.Graftingofconcentratedbonemarrowmononuclearcells(BMMC)骨髓单核细胞hasbeencombinedtocoredecompressiontotreattheearlystageofONFH,andseveralstudiesshowedpromisingresults.91,92,93,94,95,96,97Giventhatsizeandlocationofthenecroticlesionarethemajordeterminantsoffurthercollapseofthefemoralheadandcollapsedoesnotoccurinsmalllesionsevenwithoutanyintervention,19,98,99thereislimitedevidencetoconfirmtheeffectivenessofBMMCtherapyinwell-designedstudies.Thus,alarge-scalerandomizedcontrolledtrialtoverifytheefficacyofcoredecompressionwith/withoutBMMCiswarranted有必要进行一项大规模的随机对照试验,以验证髓芯减压术结合BMMC与否的有效性。Insummary,theexactpathogenesisofONFHisstillunknown.MostinvestigatorsagreethatONFHhasamultifactorialetiologybutprogressionofthediseaseoccursthroughonefinalcommonpathway,whichisdecreasedbloodflowtothefemoralheadthatleadstoischemiaandcelldeath.Attentionhasbeengiventotheinterplaybetweenindividualgeneticpredispositionsandassociatedriskfactorsthatcanpotentiallyleadtothefinalcommonpathway,butanimportantknowledgegappersistsintermsofwhenandhowthosefactorsinteracttoleadtotissueischemiaandnecrosis.Therefore,well-designedbasicsciencestudiesandhypothesis-driven,prospective,randomized,controlled,largescaleclinicaltrialsareneeded.
 曾纪洲 主任医师 北京潞河医院 骨关节外科1人已读
曾纪洲 主任医师 北京潞河医院 骨关节外科1人已读 - 髋关节的关节囊盂唇复合体:解剖、疾病、术前与术后MRI特征(2024)
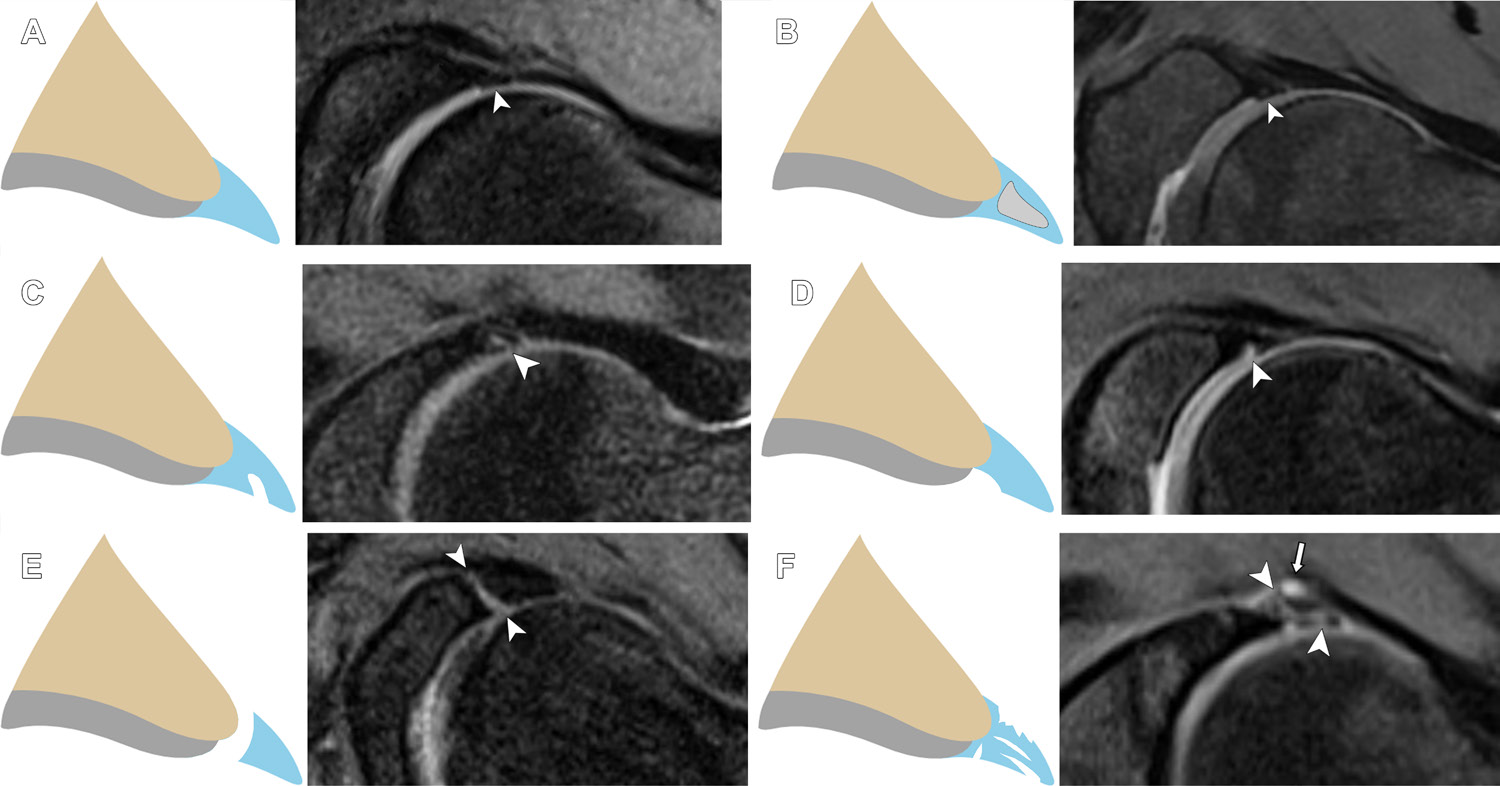
髋关节的关节囊盂唇复合体:解剖、疾病、术前与术后MRI特征(2024)HipCapsulolabralComplex:Anatomy,Disease,MRIFeatures,andPostoperativeAppearance FloresDV,FosterR,SampaioML,RakhraKS.HipCapsulolabralComplex:Anatomy,Disease,MRIFeatures,andPostoperativeAppearance[J].Radiographics,2024,44(2):e230144. 转载文章的原链接1:https://pubmed.ncbi.nlm.nih.gov/38300815/ 转载文章的原链接2:https://pubs.rsna.org/doi/10.1148/rg.230144?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed AbstractThehipisauniquelyconstrainedjointwithcriticalstaticstabilityprovidedbythelabrum,capsuleandcapsularligaments,andligamentumteres.Thelabrumisafibrocartilaginousstructurealongtheacetabularrimthatencirclesmostofthefemoralhead.Labraltearsarelocalizedbasedontheclock-facemethod,whichdeterminestheextentofthetearwhileprovidingconsistentterminologyforreporting.Normallabralvariantscanmimiclabraldiseaseandcanbedifferentiatedbyassessmentofthicknessorwidth,shape,borders,location,andassociatedabnormalities.TheLageandCzernyclassificationsystemsarecurrentlythemostwell-knownarthroscopicandimagingsystems,respectively.Femoroacetabularimpingementisariskfactorfordevelopmentoflabraltearsandisclassifiedaccordingtobonedysmorphismsofthefemur("cam")oracetabulum("pincer")orcombinationsofboth(mixed).Thecapsuleconsistsoflongitudinalfibersreinforcedbyligaments(iliofemoral,pubofemoral,ischiofemoral)andcircularfibers.Capsularinjuriesoccursecondarytohipdislocationoriatrogenicallyaftercapsulotomy.Capsularrepairimproveshipstabilityattheexpenseofcapsularovertighteningandinadvertentchondralinjury.Theligamentumteresissituatedbetweentheacetabularnotchandthefoveaofthefemoralhead.Initiallyconsideredtobeinconsequential,recentstudieshaverecognizeditsroleinhiprotationalstability.Existingclassificationsystemsofligamentumterestearsaccountforinjurymechanism,arthroscopicfindings,andtreatmentoptions.Injuriestothelabrum,capsule,andligamentumteresareimplicatedinsymptomsofhipinstability.Theauthorsdiscussthelabrum,capsule,andligamentumteres,highlightingtheiranatomy,pathologicconditions,MRIfeatures,andpostoperativeappearance. 图1 Abbreviations:FAI=femoroacetabularimpingement,ILFL=iliofemoralligament,ISFL=ischiofemoralligament,MRA=MRarthrography,PDFS=protondensity–weightedfat-suppressed,PFL=pubofemoralligament,T1FS=T1-weightedfat-suppressed TEACHINGPOINTS„ Byconvention,labraltearsarelocalizedbasedontheclock-facemethod,where3o’clockisanterior(demarcatingtheanteriorsuperiorandanteriorinferiorquadrants),6o’clockisthetransverseligament,and12o’clockisthesuperiorapexoftheacetabulum.Thiswasshowntobeanaccuratemethodthatmatchesthearthroscopist’slocalizationandimpressionoftheextentoflabraltears,therebyprovidingastandardizedmethodofreporting.„ Incontradistinctiontolabraltears,whichareirregularandextendintothelabralsubstance,themarginsofthelabrumattheinterfacewithasulcuswillbesmooth.Otherfeaturesthatfavorasulcusoverateararelessthanone-halflabralwidthfluidsignalintensitybetweenthebaseofthelabrumandtheacetabularrim;linearshape;absenceofregionalparalabral,cartilage,orosseousabnormalities;andposteriorinferiorquadrantlocation.„ Incontrasttothenativelabrum,increasedsignalintensityintheoperatedlabrumthatsurfacesisnotnecessarilyaretearandmayrepresentgranulationtissueorahealedtear.Increasedfluid-orgadolinium-intensitysignalwithinthelabrumthatsurfaces,extensionoflabralabnormalitybeyondthesutureanchorzoneorbeyondthemarginsoftheoriginaltear,paralabralcyst,andlabraldistortionaresignsofaretear.„ Capsularlesionsintheabsenceoftraumatichipdislocationmayberelatedtoopenorarthroscopiccapsulotomyorcapsulardehiscence.Intheabsenceofcapsularrepair,postoperativechangestotheadjacentstructures,capsularirregularity,edema,orafrankdefectmayindicatethesiteofarthroscopytrocarplacement.Capsulardehiscenceisapossiblecomplicationofcapsularrepair.ItisappreciatedatMRIasadisruptedordiscontinuouspseudocapsule,oftencharacterizedbyafluid-filledgapwithorwithoutassociatedpseudocapsularthickeningandhyperintensity.„ Iatrogenicinstabilityisararepostarthroscopycomplication.Osseousriskfactorsincludeexcessiveboneremovalduringacetabularrimresectionorfemoralosteoplasty.Largecapsulotomieswithoutcapsularrepairandnonhealingcapsulardefectsfrompreviousarthroscopyareexamplesofsoft-tissueriskfactors. IntroductionThehipisaball-and-socketjointconsistingofthecuplikeacetabulum,whichreceivesthesphericalfemoralhead.Itisauniquelyconstrainedjoint,inlargepartduetolarge-volumecoverageofthefemoralheadbytheacetabulum.Staticstabilityisfurtherprovidedbythreeimportantsoft-tissuestructures:thelabrum,capsuleandcapsuloligamentouscomplex,andligamentumteres(Fig1). Figure1.Graphicillustrationdepictsthecapsulolabralcomplexofthehip. Thelabrumandcapsulearecriticalcomponentsofthejoint’sstrongsuctionmechanism,maintainingtheintra-articularhydrostaticpressurenecessarytocontainthefluidwithinthecentralcompartment(1).Thecapsuleandcapsularligamentsallowafullrangeofmotionbutrestrictmovementsthatpredisposetosubluxationanddislocation.Theligamentumteresisasecondarystabilizerofthehip,supplementingthecapsularligamentsbyactingasa“sling”topreventsubluxationofthefemoralheadattheextremesofmotion.Thesize,variableform,andorientationofthesestabilizers,alongwithcloseappositionofthejoint’sarticularsurfaces,makeimagingevaluationchallenging.Furthermore,theadventofhiparthroscopyhasincreasedrecognitionofnumerouspathologicconditionsaffectingthesestructures,requiringcarefulscrutinybytheradiologist.Thisarticlediscussesthelabrum,capsule,andligamentumteres,emphasizingtheiranatomy,pathologicconditions,MRIfeatures,andpostoperativeappearance.Hipinstability,asourceofmuchcontroversyanddebate,isalsodiscussed,highlightingtheterminologyandclassification. ImagingConsiderationsConventionalradiographyremainsthefirstlineofimagingforinvestigationofallhipdisorders.Inthecontextofcapsulolabralstructures,itallowsevaluationofosseousdysmorphismsthatmaypredisposetolabraltearsorhipinstability,including“cam”and“pincer”femoroacetabularimpingement(FAI),hipdysplasia,andosteoarthritis.USisusefulinscreeningfortendondisease,muscletears,jointeffusion,andperiarticularfluidcollections.CT,withitscross-sectionalcapabilityandstrongdepictionofosseousmorphology,allowscharacterizationofhipdysplasiaandcamorpincerdeformitiesinmultiplanarandthree-dimensionalforms(FigS1).Inpatientswhoarecandidatesforjoint-preservationsurgery,italsoenablescalculationofimportantmetricssuchasacetabularandfemoralversion(2).MRIremainstheimagingtoolofchoicefordirectevaluationofthelabrum,capsularligaments,andligamentumteres(3).Optimizedprotocolsincludeadedicatedsurfacecoil,targetedfieldofview,thinsectionthickness,andhighin-planeresolutiontodepicttheanatomyanddiseaseofthesesmallstructures.Theadditionofthree-dimensionalacquisitionsthatuseisotropicvoxels(voxelswiththesamedimensionsinthex,y,andzplanes)enablesimagestobereconstructedinanyplane(4).Radialreconstructions,specifically,generateimagesorientedperpendiculartothecurvatureofthejoint,henceprovidingtruecrosssectionsofallquadrantsofthejoint.Theyareunhinderedbypartial-volumeeffects,optimizingdepictionofcartilageandthelabrum,whichisparticularlyimportantininvestigationofFAI(5).VisualizationofcapsulolabralstructuresisfurtherimprovedbycombiningMRIwithintra-articularcontrastmaterialorMRarthrography(MRA).Comparedwiththestandardofreferenceofarthroscopy,MRAexhibitsspecificity,sensitivity,andaccuracyof100%,92%–100%,and93%–96%,respectively,fordiagnosinglabraltears(6–8).Recentstudieshavedemonstratedthatconventionalornonarthrographic3-TMRImaybeadequateforevaluationofthelabrum(9–11).Astudyof38patientswithsuspectedFAIfoundaspecificityof50%butsensitivity,accuracy,positivepredictivevalue,andnegativepredictivevalueof98%–100%fornonarthrographicMRIwitharthroscopyasastandardofreference(9).Anotherinvestigationof68patientswithFAIalsofoundthatconventional3-TMRIisequivalentto1.5-TMRAfordetectinglabraltears(12).Arecentmeta-analysisfoundthatthesensitivityof3-TMRIwasclosetothatofMRA(pooledsensitivityof80%vs89%)anditsspecificitywashigherthanthatofMRA(pooledspecificityof77%vs69%)(11).Atourinstitution,conventional3-TMRIhasreplacedMRAastheworkhorseforinitialevaluationofhipinternalderangement.WereserveMRAforevaluatingapostoperativehiporyoungadultswithpersistentpainandnormalresultsof3-TMRI.MRAisthepreferredtechniquefordetectinghipcapsularandligamentumteresabnormalities(13,14).AninvestigationbyTomasevichetal(13)foundthatthesensitivityfordetectinghipcapsulardefectsafterhiparthroscopywassignificantlyhigherforMRAcomparedwithMRI(87.5%vs50%,respectively).MRAalsoshowssensitivity,specificity,positivepredictivevalue,negativepredictivevalue,andaccuracyfordetectionofligamentumterestearsof78%,97%,74%,97%,and95%,respectively(15).Theaxialobliqueplaneisparticularlyusefulfordifferentiatinggradesofligamentumteresinjuriesandimprovingspecificityfordifferentiationofpartialandcompletetears(14). AcetabularLabrumThelabrumistypicallytriangularincrosssectionandisfixedtotheacetabulumatitsbase(Fig2).Thebasehasdualattachment,spanningboththehyalinecartilage(chondrolabral)andtheacetabularbone(osseolabral).Atitschondralattachment,thelabrumstronglyadherestotheacetabularrimviaazoneofcalcifiedcartilageknownasthetidemark(16).Thechondrolabraljunctionhasavariabledegreeofblendingandevenoverlapofthelabrumwithacetabularhyalinecartilage.Thelabrumterminatesanteroinferiorlyandposteroinferiorly,whereitisbridgedbythetransverseacetabularligament.Exceptfortheregionclosesttothecapsule,thelabrumispoorlyvascularized,limitingitsabilitytohealoncetorn(17). Figure2.Normallabralanatomy.=paralabralrecess,arrowhead=osseolabraljunction,reddottedline=labralbase.(A)Graphicillustrationshowsnormallabralanatomy.(B)CoronalT1-weightedfat-suppressed(T1FS)MRarthrogramina39-year-oldhealthyasymptomaticvolunteershowsnormallabralanatomy.Yellowdottedline=tidemark. MRIoftheLabrumThenormallabrumtypicallyhasdiffuselowsignalintensitywithallMRIsequences.Intrasubstanceintermediateorhighsignalintensitycanbeseeninhealthyindividualsandmayrepresentmucoiddegeneration,fibrovascularbundles,ormagicangleartifact(3).Theanteriorsuperiorlabrumismostpronetosignalintensityvariations,includingglobular,linear,orcurvilinearshapes(18).Thelabrumisoftentriangular(66%–69%),althoughround(11%–16%)andflat(9%–13%)shapeshavebeenreported(18).Byconvention,labraltearsarelocalizedbasedontheclock-facemethod,where3o’clockisanterior(demarcatingtheanteriorsuperiorandanteriorinferiorquadrants),6o’clockisthetransverseligament,and12o’clockisthesuperiorapexoftheacetabulum(Fig3)(19).Thiswasshowntobeanaccuratemethodthatmatchesthearthroscopist’slocalizationandimpressionoftheextentoflabraltears,therebyprovidingastandardizedmethodofreporting(19). Figure3.Clock-facelocalizationoftheacetabularlabrum.Graphicillustration(A)andsagittalT1-weightedfat-suppressedMRimage(B)showclock-facelocalizationoftheacetabularlabrum.Thetransverseacetabularligament(highlightedinyellow)isassignedas6o’clock,withtheacetabulumdividedintoquadrants:3o’clockisanterior,9o’clockisposterior,and12o’clockissuperior(apexoftheacetabulum). LabralVariantsAsidefromvariationsinshapeandsignalintensity,groovesorspacesformedbythelabrumwitheithercartilage(sublabralsulci)orthecapsule(paralabralrecess)canbeconfusedwithalabraltear(18,20);theseareparticularlyconspicuouswiththedistentioneffectofMRA.Sublabralsulciarepresentinasmanyas25%ofpatientsandcanbefoundinallanatomicpositions,themostcommonbeingposteriorsuperior(48%)(Fig4)andanteriorsuperior(44%)(18).Incontradistinctionolabraltears,whichareirregularandextendintothelabralsubstance(18),themarginsofthelabrumattheinterfacewithasulcuswillbesmooth.Otherfeaturesthatfavorasulcusoverateararelessthanone-halflabralwidthfluidsignalintensitybetweenthebaseofthelabrumandtheacetabularrim;linearshape;absenceofregionalparalabral,cartilage,orosseousabnormalities;andposteriorinferiorquadrantlocation(20,21). Figure4.Sublabralsulcus.Axialobliqueprotondensity–weightedfat-suppressed(PDFS)MRimageina22-year-oldwomanwithhipdiscomfortafteranterosuperiorlabralrepairandosteochondroplastyandwithclinicalconcernforaretearshowsaposterosuperiorsublabralsulcus(arrowhead).Thereisalsoanadjacentparalabralrecess(arrow).Yellowdottedline=osseousdefectfrompriorosteochondroplasty.Resultsofarthroscopywerenegativeforalabralretear. Thejunctionofthetransverseligamentoverlappingwiththeacetabularlabrumcanalsoformanormalrecess(Fig5).Itismorecommonanteriorly(33%)andcanbeconfusedwithalabraltearoranteroinferiorlabral-ligamentousdetachment(18).Theparalabralrecessreferstothespacebetweenthecapsuleandthelabrum(Fig6)andcanbeconfusedwithaparalabralganglioncyst.Whilethecapsuleinsertsdirectlyatthebaseofthelabrumalongtheanteriorandposteriormarginsofthelabrum,itattachesseveralmillimetersabovethelabrumalongthesuperiormargin,therebymakingthisrecessmostobviousoncoronalsections(18). Figure5.Transverseligament–labraljunctionrecess.CoronalT1FSMRarthrogramina38-year-oldhealthyasymptomaticvolunteershowscontrastmaterial(arrowhead)atthejunctionbetweenthetransverseligamentandlabrum,consistentwithatransverseligament–labraljunctionrecess. Figure6.Paralabralrecess.CoronalT1FSMRarthrogramina26-year-oldfemaleasymptomaticvolunteershowscontrastmaterial(arrowhead)throughtheparalabralrecess,ananatomicspacecreatedbetweenthejointcapsuleandlabrum. LabralAbnormalitiesLabralabnormalitiesarereadilydemonstratedatMRI.Adegeneratedlabrummaymanifestwithincreasedsize,increasedintrasubstancesignalintensity,orsurfaceirregularity(22).Labraltearsoccureitherthroughitssubstanceorintheformofadetachmentofthebasefromtheadjacentacetabulum;upto90%ofcasesrepresentlabraldetachments(23).Substancetearmanifestswithincreasedsignalintensityorcontrastmaterialthroughthelabralsubstancesurfacingthearticularsurface,capsularsurface,orboth(22,23).Approximately28%oftearsmayexhibitsignalintensitylessthanthatofgadoliniumcontrastmaterialorfluid,possiblyduetoeithergranulationtissueorvolumeaveraging(24).Withlabraldetachments,increasedsignalintensityorcontrastmaterialundercutsthebaseofthelabrum,insinuatingbetweenthelabralbaseandacetabularrimeitherpartiallyorcompletely(25).Theevolutionoflabraldetachmenttypicallybeginsatthechondrolabraljunction.Intheearlieststages,theremaybeattritionoflabraltissueinthisregion,withfluidimbibitionbetweenthelabrumandhyalinecartilage—referredtoaschondrolabralseparation—orapartiallabraldetachment.Theseparationmayextendperipherallytowardthedirectionofthecapsule,resultinginadditionaldisruptionoftheosseolabraljunctionoracompletedetachmentofthelabrumfromtheacetabularrim(26).Thechondrolabraljunctionisofparticularinterestinthecontextofcam-typeimpingement,asitservesasthefirstsiteofderangementsecondarytoshearforceandcompressioninjuryofthehyalinecartilage(26).Thismayresultinchondraldelaminationleadingfromthechondrolabraljunctionandcoursinginward(26),theso-calledcarpetlesion(27).Classificationsystemsforlabraldiseaseexistinboththeorthopedicandradiologyliterature.TheLageclassificationisthemostwell-knownarthroscopicsystemandorganizeslabraltearsasflap,fibrillated,longitudinalperipheral,orunstable(28).Czernyetal(29)devisedanMRAclassificationforlabraldiseasebasedonlocation:withinthesubstance(types1and2)orattachment(type3)(Table,Fig7).Labraltearscanbesubstancetype(type2)ordetachmenttype(type3);theauthorsfoundthattypes2and3exhibitexcellentcorrelationwitharthroscopicfindings.Ontheotherhand,Blankenbakerandcolleagues(19)foundnocorrelationbetweentheCzernyandLageclassifications.TheauthorsalsorecommendeddescribingthelabralabnormalityratherthanattemptingtocorrelateitdirectlywiththeLageclassification(19). ClassificationofLabralInjuriesatMRASource.—Reference25. Figure7.RepresentativeanteriorsuperiorlabraltearsatMRAandtheirCzernyclassifications.(A)AxialobliqueT1FSMRarthrogramina20-year-oldwomanwithdailyandprogressivelefthippainshowsextensionofcontrastmaterialintothelabrum(arrowhead)withoutdetachment,consistentwithaCzernystageIIAlabraltear.(B)AxialobliqueT1FSMRarthrogramina40-year-oldwomanwithrecalcitranthipandgroinpainshowsimbibitionofcontrastmaterialintothedeformedlabrum(arrowhead),consistentwithaCzernystageIIBlabraltear.(C)AxialobliqueT1FSMRarthrogramina33-year-oldwomanwithclinicalsuspicionforlabraltearshowscontrastmaterial–filledexpansionofthelabrum(arrowhead)withdetachmentattheosseolabraljunction(arrow),consistentwithaCzernystageIIIBlabraltear. Atourinstitution,labraldiseaseisusuallyimagedusingconventional3-TMRI.Followingthisprotocolandincorporatingrecommendationsbypreviousauthors(19),weusethefollowingterminologyfordescribingcommonlabralpathologicconditions:(a)degeneration=increasedintra-substancesignalintensitywithoutsurfacing,(b)substancetear=increasedintrasubstancesignalintensityextendingtothecapsularorarticularsurfaceofthelabrum,(c)partialdetachmenttear=partial-widthincreasedsignalintensityextendingbetweenthebaseofthelabrumandacetabularrimatthechondrolabralorosseolabraljunction,(d)completedetachmenttear=increasedsignalintensitybetweenthelabrumandacetabularrimextendingacrossthefullwidthofthelabralbase,and(e)complextear=multidirectionalormultipleincreased-signal-intensitytearlines,extendingtoboththedeeparticularandcapsularsurfaces(Fig8)(22). Figure8.Normalandabnormalanteriorsuperiorlabrum.(A)Graphicillustration(left)andaxialobliquePDFSMRimage(right)ina27-year-oldasymptomaticvolunteershowanormallabrumwithhomogeneouslowsignalintensity(arrowhead),preservedtriangularshape,andsmoothborders.(B)Graphicillustration(left)andaxialobliquePDFSMRimage(right)ina36-year-oldwomanwithhippainandclinicalconcernforlabraltearshowasmallareaofincreasedsignalintensity(arrowhead)withinthelabralsubstancenotreachingasurface,consistentwithlabraldegeneration.(C)Graphicillustration(left)andaxialobliquePDFSMRimage(right)ina43-year-oldwomanwithsymptomsofimpinge-mentshowfocallinearincreasedsignalintensity(arrowhead)withinthelabralsubstancebreachingthearticularsurface,consistentwithasubstancetear.(D)Graphicillustration(left)andaxialobliquePDFSMRimage(right)ina37-year-oldwomanwithpersistenthippain,querylabraltear,showpartial-widthincreasedsignalintensity(arrowhead)atthechondrolabraljunctionnotextendingpastthechondrolabraljunction,consistentwithchondrolabralseparationorpartiallabraldetachment.(E)Graphicillustration(left)andaxialobliquePDFSMRimage(right)ina78-year-oldwomanwithsymptomsofimpingementshowincreasedsignalintensity(arrowheads)extendingcompletelyfromthechondrolabraljunctiontothelabralbase,consistentwithcompletelabraldetachment.(F)Graphicillustration(left)andaxialobliquePDFSMRimage(right)ina51-year-oldwomanwithlefthippainworsewithrunningshowmultipleincreased-signal-intensitylines(arrowheads)extendingtobothdeeparticularandcapsularsurfaces,consistentwithacomplextear.Asmallparalabralcyst(arrow)atthecapsularsurfaceisalsopresent. Chroniclabraltearanddegenerationcanresultinlabralossification,whichmayexacerbateimpingementsymptoms.AtMRI,ossificationappearsasasmallfocusofsignalintensitysimilartothatofbonemarrow(26)—althoughitmayevenbeoccult—andisthereforebestevaluatedonradiographsorT1-weightedimages(Fig9).Thepresenceofossificationshouldbereported,asitmayleadtoamoredifficultrepair,makinglabraldébridementtheoptimalapproach(30). Figure9.Completelabraldetachmentwithossificationina32-year-oldmalecyclist.CoronalT1-weighted(A)andPDFS(B)MRimagesshowasmallfocusofossification(arrowinA)adjacenttothesuperolateralacetabulumwithmarrow-equivalentsignalintensity,consistentwithossification.Thereisafluid-filledcleft(arrowheadinB)extendingcompletelyfromthechondrolabraljunctiontothelabralbase,consistentwithcompletelabraldetachment. Contrarytotearsinitsglenoidcounterpart,acetabularlabraltearsmostcommonlyoccurintheanteriorsuperiorquadrant(23).Tearsoftheposteriorsuperiorquadrant(Fig10)areusuallyseeninyoungerpatients,indysplastichips,orafteraposteriorhipdislocation(19).Posteriorinferiorlabraltears(Fig11)arerareandshouldnotbeconfusedwiththerelativelycommonnormalgrooveorsulcus,whichiswelldepictedatMRA(31). Figure10.Posteriorsuperiorlabraltearina46-year-oldwomanwithlockingandhippain.SagittalPDFSMRimageshowsincreasedsignalintensitywithintheposteriorsuperiorlabrum,consistentwithalabraltear,withanadjacentsmallparalabralcyst(arrow). Figure11.Posteriorinferiorlabraltearina48-year-oldmanwithdeeplefthippainradiatingtothegroin.Axialoblique(A)andsagittal(B)PDFSMRimagesshowafluid-filledcleft(arrowheadinA)withanadjacentcyst(arrowinB),consistentwithalabraltearwithasmallparalabralcyst. Aparalabralcystcanarisewhensynovialfluidleaksthroughalabraltearcleftandintotheperiarticularsoft-tissuespaceandbecomesencapsulated.Itaidsinrecognitionofalabraltearandisoftenlocatedintheanteriorsuperiorquadrant(32).ParalabralcystsusuallyhavelowtointermediatesignalintensityonT1-weightedimagesandhighsignalintensityonT2-weightedimages,althoughsignalintensitycanvary(33).Owingtotheirthickgelatinouscontent,theymaynotalwaysfillwithgadoliniumcontrastmaterialatMRA(22).Avastmajorityofparalabralcystsareaccompaniedbyfull-thicknesslabraldetachmenttears(94%)(Fig12);thelackofalabralteartherebyraisesthepossibilityofanotherdiagnosis,suchassynovialcyst,focalsynovitis,tumor,orpsoasbursalfluid(33). Figure12.Anteriorsuperiorlabraltearwithaparalabralcystina68-year-oldwomanwithrighthippainandanincidentalsoft-tissuemassatpreviousCT.SagittalPDFSMRimageshowsaprominentfluid-filledcleft(arrowhead)intheanteriorsuperiorlabrumwithanadjacentlargecysticmass(arrows),consistentwithacompletelabraldetachmenttearwithaparalabralcyst. FemoroacetabularImpingementFAIisawell-recognizedriskfactorinthedevelopmentandevolutionoflabraltearsandhiposteoarthritis.Itisassociatedwithanatomicalterationsthatimpairinteractionsbetweenthefemurandacetabulumduringmotionofthehipjoint,predisposingthelabrumtotearsandarticularcartilagetoprematuredegeneration.Itisclassifiedaccordingtobonedysmorphismascam(femoralside),pincer(acetabularside),oracombinationofbothtypes(mixed).Cammorphologyischaracterizedbyexcessboneorcartilageatthefemoralhead-neckjunction,diminishingthefemoralheadsphericityandhead-neckoffset.Pincermorphologypredisposestoimpingementduetoovercoverageofthefemoralheadbytheacetabulum.Itmaybefocal,asseenwithacetabularretroversion,orglobal,asisseenwithcoxaprofundaandacetabularprotrusio.Incammorphology,labralandchondraldisordersoccurpreferentiallyintheanteriorsuperiorquadrantofthejoint.Withpincermorphology,abutmentoftheanterioracetabularrimontothefemoralneckresultsinfocalimpactionandtearingoftheanteriorsuperiorlabrum,whicheventuallyextendsposteriorlyandultimatelycircumferentially(34). TreatmentandPostoperativeAppearanceLabraldiseasecanbemanagedwithconservativeorsurgicaloptions.Ingeneral,increasedlabralsubstancesignalintensitythatdoesnotbreachasurface(degenerativesignalintensity)isconservativelymanaged.Whiletheintraoperativeappearanceofthelabrum(ie,labralquality)(35)isthemostimportantoverallfactoraffectingsurgicaldecisionmaking,asurveybyHerickhoffandSafran(36)showedthatsurgeonsconsiderMRIorMRAfindingstobethemostimportantpreoperativefactor.Indicationstorepairatornacetabularlabrumandtypesoftreatmentarehighlyvariableamonghiparthroscopicsurgeons(35,36).Therearethreeformsoflabralsurgery:débridement,refixationorrepair,andreconstruction.Labraldebridementinvolvestrimmingoffrayedandunhealthytissue,potentiallyleavingviabletissuewithgoodhealingcapacity(37,38).Labralrefixationorrepairinvolvesreattachmenttotheacetabularrimusingsutureanchors(38).Substancetearsaretreatedwithdébridementwithorwithoutrepair,whilepartialorcompletedetachmentsaremanagedwithrepair.Incaseswherethereisinsufficientlabraltissuethatprecludesadequaterepair,suchasinasmallordiminutive(hypotrophic)labrumlessthan3mmwide,complextear,ormaceratedlabrum,labrumreconstructionusinganauto-orallograftcanbeperformed(38).Anormalpostoperativelabrumshouldbefirmlyaffixedtotheacetabularrimandremainintactoverthesutureanchorzone(39).Itistypicallyshorteranddiminutivebutshouldremainsmooth(40).Thesuturesthemselvesshouldbepositionedclosetotheacetabularrimbutshouldnotpenetratethesubchondralboneorthearticularcartilage(41,42).Kimandcolleagues(43)foundobliterationoftheparalabralrecessin94%–100%ofhiparthroscopyprocedures;thismaybeanormalpostoperativefindingrelatedtoadhesionsorscarring(Fig13)(43),althoughthisfindingmaybeworthreportinginthepresenceofsymptoms(43).Incontrasttothenativelabrum,increasedsignalintensityintheoperatedlabrumthatsurfacesisnotnecessarilyaretearandmayrepresentgranulationtissueorahealedtear(Fig14)(22,40).Increasedfluid-orgadolinium-intensitysignalwithinthelabrumthatsurfaces,extensionoflabralabnormalitybeyondthesutureanchorzoneorbeyondthemarginsoftheoriginaltear,paralabralcyst,andlabraldistortionaresignsofaretear(Fig15)(40). Figure13.Postoperativeobliterationoftheparalabralrecessina40-year-oldwomanwithpersistentlimitedrangeofmotionafterlabralrepair.CoronalPDFSMRimagesbefore(A)and1yearafter(B)arthroscopiclabralrepairshowobliterationofthepreviouslyintactsuperiorparalabralrecess(arrowinA)andreplacementwithill-definedintermediate-signal-intensitytissue(arrowheadsinB),mostinkeepingwithfibrosisorscarring. Figure14.Normalpostoperativelabrumina48-year-oldwomanimagedforassessmentofaretear.SequentialPDFSMRimagesatamoreanterior(A)andposterior(B)levelshowsignalintensitywithinthelabrumthatsurfacestobothcapsularandarticularsides(arrowheadsinA),whichmaybeworrisomeforaretearinanativelabrum.Thesutureanchorsareplacedclosetotheacetabularrim(arrowsinB)butdonotbreachthesubchondralboneorarticularcartilage.Arthroscopydemonstratedanintactposteroperativelabrum. Figure15.Labralretearina36-year-oldwoman.CoronalT1FSMRarthrogramshowsdistortionoftheanteriorsuperiorlabrumwithimbibitionofcontrastmaterial(arrowheads),consistentwithalabralretear. TheosseousdysmorphismresponsibleforFAIisusuallytreatedalongwiththelabraltear.Thetwomostimportantfactorstoconsiderinchoosingthetechniquearevisualizationoftheentirelesiontoachieveathoroughcorrectionorrepairwhilemaintainingthebiomechanicalfunctionofthejoint(44).Osteochondroplastyisthemostpopularmethodformanagingcamdeformitiesandinvolvescorrectiveresectionofthecammorphologyusingahigh-speedburr(Fig16)(44).AtMRI,theosteochondroplastybedappearsasasmoothdefectofvariablesizeatthefemoralhead-neckjunction(45). Figure16.Labralrepairwithsutureanchorina39-year-oldwomanwithlabraltear.(A)Intraoperativeimagebeforeresectionshowsaprominentfemoralhead-neckjunction(yellowdottedline),consistentwithcamdeformity.(B)Intraoperativeimageafterthecamhasbeenresectedshowsbonyconcavityofthefemoralhead-neckjunction(yellowdottedline),consistentwithpostexcisionchanges. Pincerlesionsaremanagedbyalabraltakedownandacetabularrimresectionfollowedbyreattachmentofthelabrumtotheacetabulumwithsutures(45).Theresectedportionappearsasadefectortruncationoftheacetabularrimwithorwithoutsuturesfromlabralsurgery(Fig17).Theappearanceoflabralprocedures,osteochondroplasty,andacetabularresectiondefectsmaybesubtle,attimesevenmimickingtheirnormalpreoperativecounterparts,necessitatingcarefulcomparisonwithpreprocedureimagesandoperativenoteswhenavailable. Figure17.Acetabularrimresectionandlabralrepairwithoutcapsularrepairina36-year-oldmanwithmixed-typeleftFAI.(A)PreoperativeaxialobliquePDFSMRimageshowsanintactanteriorsuperiorlabrumattachingtoanormalanteriorsuperioracetabulum(arrows).(B)PostoperativeaxialobliquePDFSMRimageshowsbonytruncationoftheanteriorsuperioracetabulum(arrows)andanadjacentfluid-filleddefectintheanteriorsuperiorcapsule(yellowdottedline)representingthearthroscopyportal.Alabralsutureisalsoshown(arrowheads). CapsuleandCapsularLigamentsoftheHipThehipcapsuleisacriticalstaticstabilizerofthehipandcontainsbothlongitudinalandcircularfibers(Fig18)(46).Thelongitudinalfibersarereinforcedbythreeligaments:iliofem-oral(ILFL),pubofemoral(PFL),andischiofemoral(ISFL).TheILFLorligamentofBigelowisthestrongestofthethree(46),limitingexternalrotationinflexionandbothinternalandexternalrotationinextension.Itconsistsofsuperiorandinferiorbandsthatextendfromthelowerpartoftheanteroinferioriliacspineandiliacmarginoftheacetabulumtotheintertrochantericline,formingareverse-Yconfiguration(46). Figure18.Graphicillustrationsshowtheosseousfootprints(A)andcourse(B)ofthecapsularfibersandligaments.Lightblue=superiorbandoftheiliofemoralligament(ILFL),pink=inferiorbandoftheILFL,green=ischiofemoralligament(ISFL),yellow=pubofemoralligament(PFL),orange=capsularfibers,whitebandinB=zonaorbicularis. ThePFLstabilizesthejointmostnotablyduringabduction.Itcoursesanteriorlyfromtheobturatorcrestandsuperiorpubicramustothefemoralneckadjacenttothelessertrochanter,blendingwiththeinferiorfibersoftheILFL.TheISFLcontributestojointstabilityduringextension.Itcoursesfromtheischialaspectoftheacetabularrimtothegreatertrochantericbaseposteriortothehip.ThezonaorbicularismakesupthecircularfibersandrepresentsacircumferentialcapsularthickeningattachingsuperiorlytothefemuratthebaseofthegreatertrochanterbeforeconvergingwiththesuperiorbandoftheISFL(46).Itensheathstheposteriorcircumferenceofthefemoralnecklikeaslingandformsthedistalfreeborderoftheposteriorportionofthearticularcapsule.Whileconventionallythoughttobeinconsequentialtojointfunctionandbiomechanics,recentstudieshavepostulateditsrolesinrestrainingjointdistraction(47)andcirculatingsynovialfluidbetweenthecentralandperipheralcompartments(46). MRIoftheCapsularLigamentsAtMRI,thecapsularstructureshavehomogeneouslylowsignalintensitywithallsequences.TheILFLbandsandISFLarebestidentifiedintheaxialandaxialobliqueplanes(Fig19).CoronalsectionsattheanteriorcapsuledepicttheILFL,whilesagittalsectionsdemonstratethePFL(Fig20)(48).ThezonaorbicularisisdepictedatbothMRIandMRA;intra-articulargadoliniumcontrastmaterialenhancesvisualizationoftheligamentanditssynovialfolds(49).Althoughoftendescribedasformingacollararoundthefemoralneck,itappearsasafullcircleinonly20%ofcases(49). Figure19.NormalMRIoftheILFLina26-year-oldmaleasymptomaticvolunteer.(A)AxialobliqueT1-weightedMRarthrogramatamoresuperiorlevelshowsthesuperiorbandoftheILFLinsertingontothesuperioraspectoftheintertrochantericline(arrowhead).Medially,theinferiorbandoftheILFL(thickstraightarrow)isseenasadistinctthickeningontheanteriorcapsule.TheISFLappearsasathickeningoftheposteriorcapsule(curvedarrows).Thezonaorbicularis(thinstraightarrow)isafocalprominencethatformsthedistalfreeborderoftheposteriorcapsule.(B)AxialobliqueT1-weightedMRarthrogramatamoreinferiorlevelshowstheinferiorbandoftheILFL(arrow)insertingontotheinferioraspectoftheintertrochantericline(arrowhead). Figure20.NormalMRIofthePFLina26-year-oldmaleasymptomaticvolunteer.SagittalT1FSMRarthrogramshowsanintactPFL(arrows).Theiliopsoastendonisseenintheanterioraspectofthejoint(arrowheads). Capsuleandcapsularligamentinjuriesusuallyfollowdefinitivehipdislocationsafterhigh-energycontactsportinjuriesorimpactionofthekneeagainstacardashboardwiththehipflexed(50).Thedirectionisfrequentlyposterior,wheretheheadofthefemurliesposteriortotheacetabulumandtheinjuredlowerextremityexhibitsshortening,medial(internal)rotation,flexion,andadduction(51).Onanteroposteriorradiographs,anteriorandposteriordislocationsmayappearsimilar.However,inaposteriordislocation,thefemoralheadisusuallylocatedposterior,superior,andlateraltotheacetabulum(FigS2).ThepreciseroleofMRIintreatmentalgorithmsforacutehipdislocationisnotclearlydefined,butitmaybeusefulinearlyrecognitionofsoft-tissueinjuries(Fig21)(52)anddetectionofintra-articulardamagesuchaschondralinjury,labraltear,ormissedintra-articularbody(53).Theimagingtriadofposterioracetabularlipfracture,ILFLdisruption,andhemarthrosiswasfoundtobepathognomonicofposteriorhipdislocationinacaseseriesofeightfootballplayers(54). Figure21.HipdislocationatMRI.AxialT1FSMRarthrogramina23-year-oldwoman3daysafterareportedposteriorhipdislocationshowsaprominentdefectintheISFL(arrowheads)consistentwithacompletetear,withextravasationofcontrastmaterialintothesofttissues(arrows). Anteriordislocationisfarlesscommon,occurringinlessthan8%oftraumatichipdislocations(52).Themechanismofinjuryisforcedhipabductionandexternalrotation;thefemoralheaddislocatesanteroinferiorlywhenthehipisflexedandanterosuperiorlywhenthehipisextended(52).Thetransverseligament,ligamentumteres,posteriorcapsule,andPFLmaybeinjuredinanteriorinferiordislocations(52).Dataonanteriorsuperiordislocationsarelimited,althoughinjuriestotheligamentumteres,ILFL,andsuperiorcapsulehavebeenreported(52). PostoperativeAppearanceCapsularrepairortighteningprocedureshaveyettogainuniversalacceptanceamonghipsurgeons,eventhoughavastmajorityofhigh-volumearthroscopistsrecommendthemforcapsularredundancyorlaxityorafterarthroscopy(55).Theseproceduresimprovehipstabilityanddecreasetheriskofpostoperativehipdislocationattheexpenseofiatrogenicfemoralheadchondraldamage,capsuleovertightening,andhipinfectionduetolongerexposuretime.Capsularrepairorplicationusessuturestoclosethecapsular“barearea”atthesiteofpriorarthroscopy.Itisrecommendedforcapsularredundancy,symptomaticcapsularlaxity,orgeneralizedligamentouslaxityduetoanunderlyingconnectivetissuedisorderorafterarthroscopy(56).AtMRI,therepairedcapsuleisusuallysignificantlythickerthroughtheILFLatthesiteofroutinecapsulotomyandclosurecomparedwiththecontralateralnonoperativehip(57).Othercapsulartighteningproceduresarethermalcapsulorrhaphyandcapsularreconstruction(50,56).Capsularlesionsintheabsenceoftraumatichipdislocationmayberelatedtoopenorarthroscopiccapsulotomyorcapsulardehiscence.Intheabsenceofcapsularrepair,postoperativechangestotheadjacentstructures,capsularirregularity,edema,orafrankdefectmayindicatethesiteofarthroscopytrocarplacement(Fig22).Capsulardehiscenceisapossiblecomplicationofcapsularrepair.ItisappreciatedatMRIasadisruptedordiscontinuouspseudocapsule,oftencharacterizedbyafluid-filledgapwithorwithoutassociatedpseudocapsularthickeningandhyperintensity(58).Spontaneoushealingofthecapsulecanbeseenasearlyas6weeks,dependingonthearthroscopicapproach(Fig23)(59). Figure22.Postarthroscopycapsuledefectina41-year-oldwomanwhounderwentrecentlabralrepairwithoutcapsularrepair2weeksearlier.CoronalT1FSMRarthrogramshowsawell-demarcatedcontrastmaterial–filleddefectoftheILFL(arrowhead)withsurroundingsusceptibilityartifacts,consistentwithapostarthroscopycapsuledefect Figure23.Capsularhealingina46-year-oldmanwithpersistentimpingementsymptomsaftersurgery.(A)PostoperativePDFSMRimage2weeksaftercapsulectomyandosteochondroplastyshowsanewlyexcisedfemoralhead-neckjunction(arrow)withoverlyingill-definedsoft-tissueedema(arrowheads),consistentwithcapsulectomychanges.(B)PostoperativePDFSMRimage5.5monthsaftertheprocedureshowsintervalresolutionoftheedemaandfillinginofthecapsule(arrowheads),consistentwithcapsularhealing. LigamentumTeresTheligamentumteresisatubularligamentsituatedbetweentheperipheralinferioracetabularnotchandthefoveaofthefemoralhead.Itarisesfromthetransverseacetabularligamentalongtheinferiormarginoftheacetabulumandattachestotheperiosteumofthefoveabytwobands:ischialandpubic.Awarenessandinterestintheligamentumtereshaveincreasedwiththeexpansionofhiparthroscopy.Initiallyconsideredaninconsequentialvestigialstructure,recentstudieshaverecognizeditsroleinfemoralheadvascularity,proprioception,nociception,androtationalstabilityofthehip(14).Martinandcolleagues(60)describeditsroleinhipstabilityusingaball-and-stringmodel(Fig24). Figure24.Graphicillustrationsdemonstratethemechanismofhipstabilityprovidedbytheligamentumteres,accordingtotheballand-stringmodel.(A)Asthehipjointisabducted,theligamentumtereswrapsunderthefemoralheadwhilepullingitintotheacetabulum,limitinginferiorsubluxation.(B)Asthehipjointisexternallyrotated,theligamentumtereswrapsaroundthefemoralheadwhilepullingitintotheacetabulum,limitinganteriorsubluxation. MRIoftheLigamentumTeresLigamentumteresinjuriesareassociatedwithhipdislocation,flexion-adductionstress(ie,fallonipsilateralkneewiththehipflexed),orabruptexternalrotationofthehipsuchasintwisting(14).Variousclassificationsystemshavebeenproposed(61).GrayandVillar(62)firstclassifiedinjuriesbasedoninjurymechanismaswellasarthroscopicfindings.TheDombclassificationwasdevelopedtoquantifythedegreeofligamentruptureintype2lesionsorpartialtears(63).PorthosSalasandO’Donnell(64)proposedathirdclassificationtofurtherdelineatethecauseofthetearandincorporatetreatmentoptions.Finally,O’DonnellandArora(65)accountedforligamentouslaxityinadditiontotheligament’sappearance.AtMRI,theligamentappearsasasmooth,predominantlyhomogeneous,andlow-signal-intensitystructurewithallpulsesequences.Itisbestdepictedonaxialandcoronalimages,appearingasabilobedslightlystriatedligamentcomprisedofonetothreebundles(Fig25)(14,66).Ithasanaverageoveralllengthof28mmandmeasuresapproximately3–4mminthickness,graduallytaperingfromproximaltodistal(66).Slightlyincreasedsignalintensitynearitscurvedattachmenttothefoveacapitisfemorisonshortertimetoecho(TE)–basedimagesmaybeattributabletothe“magicangle”artifact(14). Figure25.NormalMRIoftheligamentteresintwopatients.(A)CoronalT1FSMRarthrogramina24-year-oldfemaleasymptomaticvolunteershowsanormalsinglebundleoftheligamentumterescoursingfromthefoveacapitis(arrowhead)tothetransverseacetabularligament(arrow).(B)CoronalT1FSMRarthrogramina30-year-oldfemaleasymptomaticvolunteershowsanormaldoublebundleoftheligamentumterescoursingfromthefoveacapitis(arrowhead)tothetransverseacetabularligament(arrow). Partialandcompletetearsaremostcommoninthefoveacapitis;thoroughinspectionofthisregionisthereforeimportant(14).WhileMRAhasbeenshowntobeaccurateindiagnosingligamentumterestears,literatureontheaccuracyofconventionalMRIissparse.AnintactligamentandapartiallytornligamentcanhavesimilarimagingfindingsatMRA,makingdiagnosisofpartialligamentumterestearsdifficult(66).Highsignalintensitywithinthesubstanceofthefibersandperipheralirregularityaresuggestiveofapartialtear(Fig26)(66).Acompletetearmanifestswithfull-thicknessfiberdiscontinuityandligamentlaxity. Figure26.Partialtearoftheligamentumteresina29-year-oldfemalesprinterwith4weeksofgroinpain.CoronalPDFSMRimageshowsfocaldiscontinuityofthesuperiorandmedialfibers(arrowhead)oftheligamentumteres,consistentwithapartialtear. AnondisplacedfracturefragmentmayaccompanyeitherapartialorcompletetearbutmaybeoverlookedatMRI,requiringcarefulevaluationofmarrowsignalintensityonprotondensity–weightedfat-suppressed(PDFS)orT2-weightedimages(14).ConventionalCTorCTarthrographymaybemoreoptimalforevaluatingfragmentscomparedwithMRIorMRA(Fig27).Achronicallytornligamentiselongated,irregular,lax,orattenuatedwithfibersremainingcontiguous.Absenceofedemaintheacetabularfossa,synovitis,andjointeffusionallowdistinctionofchronicfromacutetears(Fig28)(14). Figure27.Acuteavulsionfractureoftheligamentumteresina22-year-oldmanafterlefthipdislocation.(A)CoronalPDFSMRimageshowsanacuteavulsionfractureofthefovealattachmentoftheligamentumteres(arrowhead)andassociatedmarrowedemaintheacetabulum(arrows).(B)CoronalCTimageshowsasmallavulsedfragment(arrowhead).Thereisalsoanundisplacedfractureoftheadjacentmedialwalloftheacetabulum(arrow). Figure28.Chronictearoftheligamentumteresina45-year-oldformerbasketballplayerwith6yearsofinguinalpainexacerbatedbysquatting.CoronalPDFSMRimageshowsmarkedthickeningoftheligamentumteresatthefoveacapitis(arrowheads)withpreservedfibercontiguity,consistentwithachronictear. TreatmentComparedwithtreatmentsforlabralandcapsuledisease,therearelimiteddataonmanagementofligamentumteresinjuries.Formostcases,conservativemanagementisadequate.Tearsarecurrentlytreatedarthroscopically(67),andindicationscontinuetoevolve.Currentindicationsarepain,instability,andmechanicalsymptomswithMRIfindingsofligamentthickening,partialorcompletetears,oravulsionfractureoftheligamentwithintra-articularosteochondralfragmentsandedemaintheacetabularfossa(14).Treatmentoptionsareshrinkage,débridement,andmostrecentlyreconstruction.Shrinkageanddébridementarereservedforpartialtearsafterfailedconservativemanagement.Fibroblasticresponsefromthermalshrinkageimprovesthebiomechanicalstrengthoftheremainingfibers,whiledébridementoffrayedandthestumpoftornfibersrelievesmechanicalsymptomsandpain(14).Reconstructionwithallografts,autografts,orsyntheticgraftsisindicatedforcompletetearsthatareconsideredreparable,causeinstability,orfailedpreviousdébridement(67). HipInstabilityHipinstabilityisabroadtermusedtodescribevariousabnormalitiesmanifestingwithdeep-seatedpainaroundthehip,groin,oringuinalregion.Thetermhasbeenusedinterchangeablywithjointhyperlaxityorhypermobilityandmicroinstability(68).Awarenessoftheentityhasincreasedrecently,althoughitsdiagnosisandevenitsexistencearestilldebated.Disordersofthecapsulolabralstructureshavebeenimplicatedinsymptomsofhipinstability.Anexhaustivediscussionisbeyondthescopeofthisarticle,butthissectionwillemphasizecurrentclassificationandterminology.Hipinstabilitymaybe(a)duetoasingleacuteepisodeoftrauma,(b)duetooveruseorrepetitivemicrotraumainayoungorathleticpatient,(c)iatrogenicinthesettingofpriorarthroscopyandcapsulotomy,(d)developmentaloranatomicsuchasinhipdysplasiaorconnectivetissuedisorders(ie,hyperlaxity),or(e)idiopathicormicroinstabilitywhentheclinicalpresentationisvagueorintheabsenceofthepreviouslymentionedcriteria(68).Traumaticinstabilitysecondarytoanacutedislocationeventmaybedistinguishedfromoveruseinstabilityonlywithareliableclinicalhistoryandphysicalexamination.Iatrogenicinstabilityisararepostarthroscopycomplication.Osseousriskfactorsincludeexcessiveboneremovalduringacetabularrimresectionorfemoralosteoplasty(FigS3).Largecapsulotomieswithoutcapsularrepairandnonhealingcapsulardefectsfrompreviousarthroscopyareexamplesofsoft-tissueriskfactors(56,69).O’Neilletal(70)describedagradingsystemforcapsularchangesatMRAinpatientswithsymptomaticpostsurgicalhipinstability.Thissystemincludesnormalcapsularappearanceandvolume,increasedcapsularredundancy(Fig29),focalcapsularrentorcapsularirregularity,andgrosscapsulardefect.Intheircohortof31patients,nocapsulesappearedcompletelynormalaftertheprocedure(70).Contrarytotraumatichipinstability,postarthroscopicinstabilityismostoftenanterior(theanteriorlateralcapsulebeingthemostcommonportalforarthroscopy)andoccurswithhipextensionandexternalrotation(71).DevelopmentaloranatomicinstabilityisseeninpatientswithdysplastichiporFAI,connectivetissuedisorders,orhypermobilitysyndromes(Ehlers-DanlosorMarfansyndrome).Thealteredbonearchitectureintheseconditionspredisposestoearlychondropathyandlabraltearsintheabsenceoftrauma,athleticactivity,orsurgery.Finally,idiopathicinstabilityormicroinstabilityreferstopainfulextraphysiologichipmotionwithoutovertsubluxationordislocation(42).Whilecausesofmicroinstabilitycanbethesameasoroverlapwiththoseofthetypesmentionedearlier,itisoftenseeninpatientswholackadefiniteunderlyingcause.Asaresult,diagnosisreliesonathoroughclinicalhistory,physicalexamination,andimagingevaluation.Currently,therearenopathognomonicimagingfeaturesofmicroinstability.Arecentsystematicreviewfoundthatintheappropriateclinicalcontext,hipdysplasia,anteriorlabraltears,andligamentumterestearsmaybesuggestiveofmicroinstability,althoughtheauthorsrecommendfurtherstudies(42).Capsularlaxityisimplicatedinmicroinstabilitybutisnotadiagnosisperse(72).Itisatermusedtodescribetheinabilityofthejointtodelivernormalresistancetoexternalforces(72).Theterminologyisoftenusedinbiomechanicalandclinicalstudies.althoughafewinvestigationssuggestimagingcorrelates.Aprospectivestudyof100consecutivepatientsshowedlowerhypermobilityscoresinsubjectswithacapsularthicknessofgreaterthanorequalto10mm(73).AnotherstudybyMagerkurthetal(74)concludedthatawidenedanteriorhipjointrecess(>5mm)andathinnedanteriorjointcapsule(<3mm)correlatewithintraoperativefindingsoflaxity. ConclusionThehipisauniquelyconstrainedjointwithcriticalstaticstabilityprovidedbythelabrum,capsuleandcapsularligaments,andligamentumteres.Understandingtheanatomy,patternsofinjury,MRIfeatures,treatment,andpostoperativeappearanceallowsprecisediagnosisandtimelymanagement.
 曾纪洲 主任医师 北京潞河医院 骨关节外科1人已读
曾纪洲 主任医师 北京潞河医院 骨关节外科1人已读
问诊记录 查看全部
- 腰痛伴双下肢疼痛半年。 患者半年来持续腰痛,尤其在起床和行走时表现明显。初期由于腰部... 结合老人年龄,此病有无解决办法,怎么提高老人生活质量。总交流次数10已给处置建议
- 外伤致左膝疼痛1月。 1个月前,患者因外伤导致左膝关节疼痛,活动时疼痛加重。当地医... 想看看用什么药?怎么治疗比较好。总交流次数7已给处置建议
- 左腹股沟疼痛2年。 患者于2年前开始出现左侧腹股沟内疼痛,疼痛性质为持续隐疼,偶... 左侧腹股沟疼痛是否是髋关节的问题,到底是否需要手术,这几天大腿跟着突然乏力发软,感觉酸,使不上劲儿,...总交流次数112已给处置建议
- 右膝关节疼痛一月余 一个多月前无明显诱因出现右膝关节疼痛症状可能与生完孩子经常抱... 这个诊断报告有什么问题吗总交流次数7已给处置建议
- 左侧膝关节疼痛两个月。 患者两个月前无明显诱因情况下出现左侧膝关节疼痛,久坐或弯曲时... 怎么能好呢总交流次数79已给处置建议
总访问量 12,893,782次
在线服务患者 9,764位
科普文章 1,221篇